Imagine that you’re in your third trimester of pregnancy, and you’re hungry or sleepy a lot of the time. It’s evening, not “time for bed” yet, but you’re sleepy, so you turn in early. And then you can’t get to sleep. You change your position and shift your pillow and covers and turn on the white noise, you count sheep and try to meditate, and finally you watch a movie or read until you fall asleep. Around 3 am, or maybe 4, you wake up hungry. You forgot to put a snack by the bed, so you get up, pee, and get something to eat. Happily you wake up only once that night; the night before, you made 3 trips to the bathroom.
In other words, you went to bed because you were tired, not on someone else’s timetable. When you couldn’t sleep you chose from an assortment of “self-soothing” techniques, each of which required a problem-solving thought process. You shifted your position when you wanted, ate when you wanted, and woke at different times from the night before.
A small baby can do every single one of those things too, but only with a caring and responsive support system, which is usually Mama. The Mama-support-system has arms that help with shifts in position. It has warmth, comfort, and reassuring sounds. It has a snuggly breast that offers food, comfort, and sleep-encouraging hormones; and it has an adult brain that does the problem-solving. The problem-solving may go something like this: Breast? No. Position? No. Diaper? No. Try breast again? Yes. Take away that responsive, problem-solving support system and you have a baby who’s totally helpless.
In fact, you have a baby who is at risk.
When babies sleep alone
This is from the American Academy of Pediatrics (AAP) current safe infant sleep recommendations:
It is recommended that infants sleep in the parents’ room, close to the parents’ bed, but on a separate surface designed for infants, ideally for the first year of life, but at least for the first 6 months. There is evidence that sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%.[1]
That’s the same as saying that having a separate-room sleeping arrangement doubles a baby’s nighttime SIDS risk. Many health professionals (and authors of nursery décor articles) are unaware of this official pediatric recommendation and the safety reason behind it.
The AAP advises against the use of home breathing and heart rate monitors,[2] and standard baby monitors and cameras have not been shown to reduce that increased SIDS risk. So while “the baby’s room” can store the toys and supplies, it’s not a safe place for an infant to sleep alone at night.
The typical sleep-training program assumes that the baby will sleep in a separate room, which runs counter to this major AAP safe infant sleep recommendation.
As to where in the parents’ room the baby should be, the AAP strongly encourages a separate surface within easy reach of the bed. But its most recent recommendations take into account the reality of tired mothers:
… the AAP acknowledges that parents frequently fall asleep while feeding the infant. Evidence suggests that it is less hazardous to fall asleep with the infant in the adult bed than on a sofa or armchair, should the parent fall asleep… Because there is evidence that the risk of bed-sharing is higher with longer duration, if the parent falls asleep while feeding the infant in bed the infant should be placed back on a separate sleep surface as soon as the parent awakens.[3]
A commercial “sidecar” that fastens to your bed is a simple way to arrange that. It provides a separate bassinet-sized surface for the baby, and you can move your baby back and forth without even sitting up.
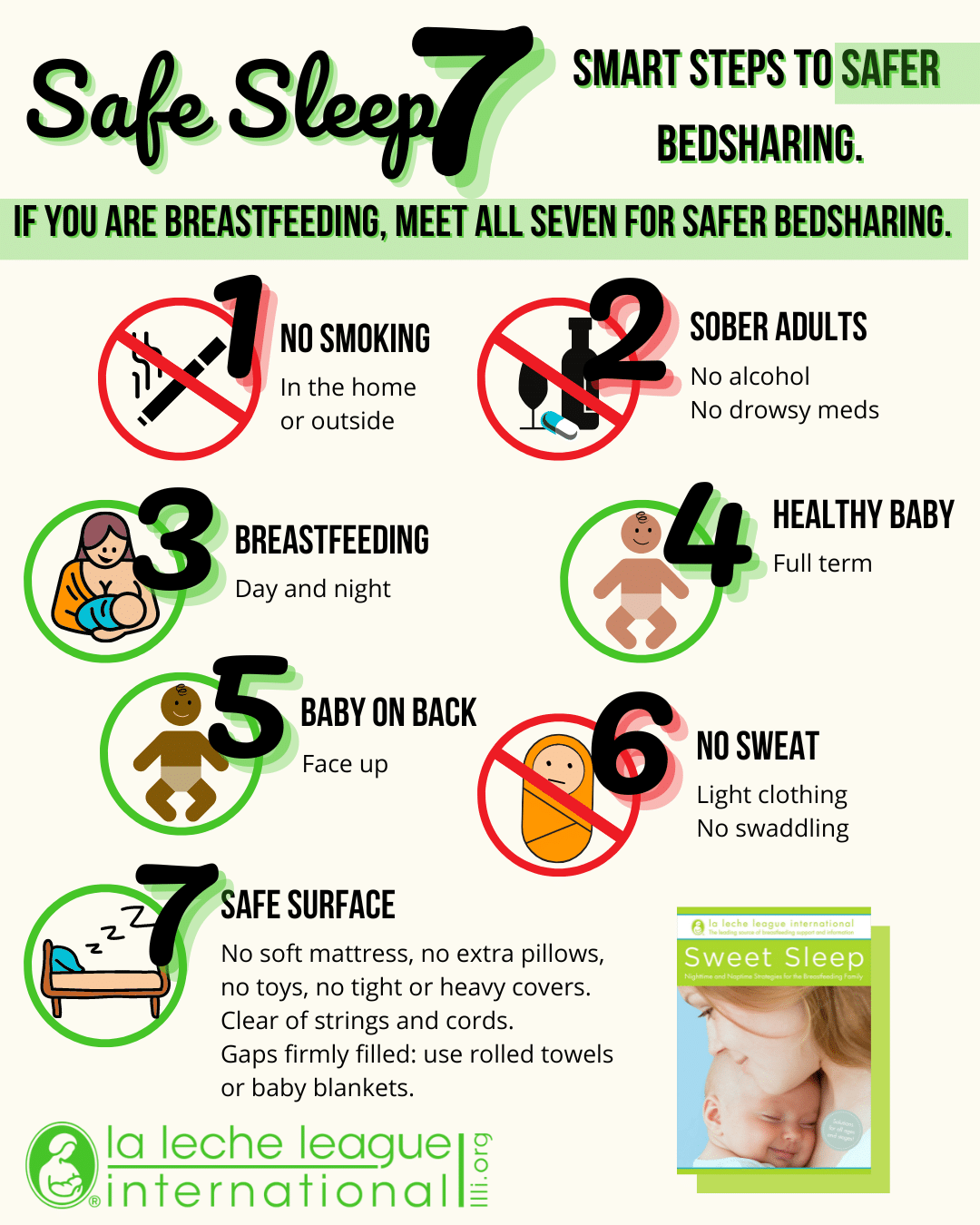
But how do you make your bed as SIDS-safe and suffocation-safe as you can for those times when you drift off? La Leche League proposes following the Safe Sleep Seven.[4] When you apply those standards to your own bed you’ve made the risk of SIDS “vanishingly small” (in one infant sleep researcher’s words) and have hugely reduced any suffocation risks.
The Safe Sleep Seven
- A non-smoking mother (and preferably household)[5]
- A sober mother (not taking medications or alcohol that affect the awareness that we normally have, awake or asleep)[6]
- Nursing freely day and night
- A healthy baby
- Baby on his or her back when not nursing[7]
- Baby not overheated,[8] and unswaddled to allow free movement
- A safe surface
What’s a safe surface?
- Firm enough that the baby can lift his head free and can’t roll into the mother’s “mattress valley”
- No sharp edges, no cords or strings that could tangle
- No gaps that could trap the baby
- Baby not too close to the edge of the bed
- No heavy covers that will drape over the baby’s head, or soft pillows that the baby might push into
Why is having a breastfed baby one of the seven standards? Formula-fed babies are already at double the risk of SIDS,[9] and in bed with their mother they may also be more prone to suffocation. Breastfeeding mothers naturally assume a “cuddle curl” position in bed, with the mother on her side and the baby in the protected “cove” between her upper arm and her thigh. And the breastfed baby naturally wants to stay there.[10] Those same behaviors aren’t automatic with a bottle-feeding mother and baby. (If your baby receives some bottles but prefers your breast, and if you naturally position your baby in that protected side-lying cove, you meet the breastfeeding Safe Sleep Seven standard.)
You’ll find more details on the Safe Sleep Seven in the first two chapters of La Leche League International’s Sweet sleep – nighttime and naptime strategies for the breastfeeding family[11], and there’s a Safe Sleep Seven infographic online here and below.)
The physiology of shared and solitary sleep
One of the delicious things that happens when your baby is close at hand is that your sleepings and wakings tend to synchronize,[12] so that you’re not startled unexpectedly from a deep sleep by a sharp cry. And your semi-conscious kissing, stroking, and covers-adjusting provide your baby with frequent stimulation. Problems with the baby’s arousal system may be a factor in some SIDS cases;[13] it may be that those normal mini-arousals are especially important for susceptible babies.
Research shows that when mothers and babies sleep far apart, even if the mothers still get out of bed to respond to the baby:
- Babies may sleep more deeply than normal, which may not be the safest sleep for them.[14]
- Babies waken less often[15] but their overall stress level may be higher[16] and they do significantly more nighttime crying.[17]
- Mothers waken less often but they waken more completely, stay awake longer, and get less sleep overall.[18]
Breastfeeding itself can be disrupted when mothers and babies are separated. Babies normally get about a third of their calories at night; spacing out nursings reduces that intake. If daytime nursings don’t compensate, milk production is reduced. Separate sleeping arrangements are linked to early weaning. [19] So is sleeping through the night.[20]
Separation and sleep-training research
Studies by sleep-training program authors do find that the programs tend to work. But the studies don’t necessarily count those families who abandon the program because the parents can’t tolerate it.[21] And they don’t tend to examine the physiological or emotional cost to the baby or the effect on breastfeeding. One independent study measured levels of cortisol, a stress hormone, during the first month and found that nighttime separation was linked to some poorer daytime coping skills in the baby.
Infants with a solitary sleeping arrangement in their first month of life showed a heightened cortisol response to the bathing session at 5 weeks compared to infants that coslept regularly. This effect was not explained by breastfeeding practices, maternal caregiving behavior, or infants’ night waking and sleep duration.[22]
In other words, mother-baby separation at night during the first month was linked to a stronger stress reaction to at least one form of routine daytime stress.
But those were young babies. There is a cost to older babies as well. One study involved 4-to-10-month-old babies who underwent a 5-day sleep-training program. The study measured the cortisol levels of mother and baby.
As expected on the first day of the program, mothers’ and infants’ cortisol levels were positively associated at initiation of nighttime sleep following a day of shared activities. Also, when infants expressed distress in response to the sleep transition, mother and infant cortisol responses were again positively associated. On the third day of the program, however, results showed that infants’ physiological and behavioral responses were dissociated. They no longer expressed behavioral distress during the sleep transition but their cortisol levels were elevated. Without the infants’ distress cue, mothers’ cortisol levels decreased. The dissociation between infants’ behavioral and physiological responses resulted in asynchrony in mothers’ and infants’ cortisol levels.[23]
In other words, mother and baby were both measurably stressed in those first few days of training. The baby stopped calling for the mother within a few days. The mother, not hearing cries, stopped being stressed by the separation. But the baby’s stress continued. It’s just that no one could hear it.
A baby’s only defense against danger is to be sheltered by an adult. Babies have a two-mode “defense program”, which plays automatically when they’re distressed and normally brings an adult running.[24] In their protest mode they cry. If that doesn’t bring help they eventually go into their “power saver” despair mode and stop crying in order to save calories, although their level of stress hormones stays high. They alternate their protest mode and despair mode as long as they can, like an intermittent distress signal.
There is no sleep-training research yet to indicate whether or not the finally-quiet baby is running the despair program or has moved past the stress of being ignored. But there’s just plain very little sleep-training research. What research does tell us is that crying causes negative changes in a baby’s physiology, from blood pressure to how well the baby can breathe. In fact,
As early as the 1980s, child development specialists encouraged caregivers to answer infant cries swiftly, consistently, and comprehensively, to eradicate the source of the infant’s distress and stop the physiologically harmful act of crying”.[25]
One interesting study that began decades ago[26] looked at the emotional health of 8-month-old babies decades later, when the babies were 34 years old. The mothering style of the 8-month-olds was rated as negative, occasionally negative, warm, caressing, or extravagantly affectionate. The adults with the least emotional distress and anxiety were those whose mothers were “caressing” or “extravagantly affectionate.” There is no mention of nighttime parenting styles in the article. Still, the article comments that “Animal research on nurturing and social bonding suggests that the neurohypophyseal hormone oxytocin may serve a crucial function in creating a powerful bond between mother and child, while disruptions in this bond can lead to dysregulation of brain chemistry and, specifically, the baby’s stress response.” In other words, interfering with the normal development of the mother-baby bond can actually change the baby’s brain chemistry.
These are just a few of the studies on the importance of mother-baby synchrony and physical proximity. But virtually every biology-related study that has looked at the mother-baby bond finds negative physiological changes – some of which may be long-term – when that normal bond is disrupted.
Our own instincts fight the notion of leaving a baby alone, even if we’ve never heard of SIDS or suffocation or physiology. Mother-wisdom is built into us, and tends to work very well indeed. But how does sleeping through the night ever happen, if babies aren’t taught how?
Normal infant/child sleep
- Newborns have a free-running clock – frequent waking night and day – while they do the fastest growing of their lives.[27]
- An infant’s total daily sleep requirement varies from baby to baby – one study found a range of 9 to 19 hours![28] – and there’s no way to predict how much sleep your own baby will need.
- Sometime between one and 4 months, babies begin to consolidate their sleep,[29] connecting short separate sleeps into longer segments. The mother’s rhythms help establish the baby’s rhythms.[30]
- By 3 months about 2/3 of babies have made a start on consolidating their sleep, though half of those backslide.[31] (Biology is almost always 2 steps forward, one step back.)
- By a year, about half of babies still need a parent’s soothing at least once a night on most nights.[32]
- Most researchers define “sleeping through the night” as sleeping from midnight to 5 am.[33]
- Given the percentage of babies that don’t sleep through the night, and the negative effect that unbroken sleep has on breastfeeding, one study suggested that mothers would benefit from a more realistic expectation of normal infant sleep.[34]
- Teenagers can sleep through anything, whether or not they underwent sleep-training.
That’s all well and good, but are there ways to slide your baby closer to the teenage nighttime coma a little faster? Well, sort of.
Sleep-nudging: Edging your child toward consolidated sleep in a kinder, gentler way
Babies’ sleep patterns vary hugely, but overall, consider your under-six-month-old to be basically unnudgeable. Young babies work all by themselves, to the extent that they’re able to, to sort out day and night and create longer intervals between nighttime nursings. But there are some ideas that may help both you and your baby through that first half-year or so.
In general:
- Get more rest during the day. Sleep isn’t something you can short-change indefinitely. So consider your naps an essential contribution to better nights.
- Learn to nurse lying down. It’s a basic survival skill for new mothers. But practice during the day; 2 am is no time to learn a new skill. (Use your pre-planned bed, not a sofa; sofas can be a suffocation risk if you fall asleep practicing.)
- If your baby is in daycare, remember that nighttime closeness and body contact are an important way to reconnect and keep your milk production up. Nighttime nursings are much more than just calorie transfer.
Some before-bedtime ideas:
- Save your must-do’s for earlier parts of the day. You and your baby are both likely to sleep better if you take some time to unwind before bedtime.
- Wear your baby for a leisurely evening stroll around the block, or even just to step out the door and take a few deep breaths. There’s something magically calming for both mother and baby about spending some time outside.
- Carry that winding-down through with a more relaxed half hour before bed. Go to bed earlier (yes, you really can). Don’t try to accomplish everything you did before babycare started taking a huge chunk out of your day. Winding down at the end of the day is almost as valuable as actually being asleep.
- Keep your baby nearby as you end your day; the noises and conversations of ordinary life tend to help a baby sleep.
- Do plenty of baby-holding before bedtime. Leaning back with your baby’s front resting against your chest releases calming hormones in both of you.[35]
- Take full advantage of those nursing hormones and nurse your baby to sleep. No, it isn’t spoiling; babies are designed to fall asleep at breast.[36] And it’s just possible that the extra milk at bedtime will stretch the interval a bit.
- Nurse your baby on a thin pad and lay him down still on that pad. The fact that the surface doesn’t change may help.
- If you hold your baby for 20 minutes or so after those eyes close, there’s a much better chance they won’t fly open again as soon as you lay your baby down.
By six months or so, but on a timetable unique to each baby, actual nudging becomes possible. But remember that most things in life are two steps forward, one step back. If you nudge too hard, just back off and try again later. Some gentle nudges:
- Keep all of the above suggestions in your repertoire.
- Start a predictable bedtime routine – “brushing” gums or teeth with a wet washcloth, reading together, singing favorite songs, all quietly and in the same order.
- Nudge toward shorter nursings:
- Slip a finger into the corner of your asleep-or-nearly-asleep baby’s mouth to slide your nipple out, maybe leaving your finger in your baby’s mouth for more sucking.
- Roll your baby over and “spoon” together after a shorter nursing.
- Nudge toward fewer nursings:
- Wear something that’s harder to get your breast out of, giving reassurances while you delay the nursing slightly. It’s a way of saying, “I’m here, but nursing takes some prep time.” Your older baby may decide it’s not worth the wait and settle for a snuggle.
- Reach across for some stroking and “shushing” when you sense your baby rousing. Sometimes it’s enough to prevent complete waking. Sometimes not.
- Roll over and turn your back after nursing. You’re still there, but your breast isn’t.
- If you have a partner, have them do the patting, singing, holding, spooning.
- Leave home briefly in the evening – starting with just a few minutes outside and increasing it over time to, say, a grocery run – and have your partner/family member do the gentling down to bedtime. Babies and small children are very good at sorting out pretend from reality, and if you’re in the house they’ll know. Just don’t stay away long at first. It can help your baby or child recognize that an alternative to your presence can be its own kind of nice, which can carry over to middle-of-the-night soothings.
- 9 month olds typically go through a more-frequent-waking stage.[37] It’s a temporary – and perfectly normal – set-back in your quest for fewer wakings.
As your child’s understanding grows, you can add some logic to the nudging:
- Nurse for a few minutes once your baby/child is in bed, and then stop nursing and move away briefly, explaining that you need to get a tissue or put something away, then come right back and offer to continue. Gradually, those breaks can get longer, you can leave the room, and at some point your little one will be asleep by the time you’ve taken the clothes out of the dryer or washed the pots and pans, trusting that you’ll return. But during the process, always keep your promise and come back. That’s what makes you trustworthy.
- Explain that the two of you nurse in daytime but only once (or not at all) at night.
- Have a nursing song that you sing at night nursings, and stop nursing when the song ends (though some little ones catch on and say, “Don’t sing!”)
- Consider a mattress on the floor near your own bed.
- If your child-who-can-walk sleeps in a separate room, you can have a daytime talk about the child doing the nighttime traveling instead of you. At some point your child won’t feel it’s worth the effort and will go back to sleep.
Some families may find it simplest and most reassuring to share a room well beyond that first year. If you find yourself edging into that approach as you go, don’t worry about what Grandma or your friend thinks. Mothers and children have shared sleep around the world and across time. And every child eventually moves on.
Your first baby-proofing
Given the risks, infant sleep-training programs that involve a separate room or deliberate inattention just aren’t a responsible choice. And decades of research have shown that, far from causing spoiling, being responsive to your baby provides a secure base for future well-being.
You know your family best, of course, and you’ll form your own unique path as you go. But no matter what a family decides about nighttime parenting, basic “baby-proofing” for every new baby needs to include
- providing a separate safe baby space in the mother’s room,
- keeping the baby close at hand in the same room at night for at least the first six months, preferably for a year, and
- making the mother’s own bed as safe as possible against accidental dozing during feedings.
Once you get the early mothering kinks worked out (and we all have them), you’ll probably look back on babyhood as one of the glory times in motherhood. Nothing to teach, nothing to discipline. Insisting on homework before dinner? Years away. Making it clear that the cat’s tail is off-limits? Not an issue. All your baby needs to do is grow and trust. And all you need to do is nurture and be trustworthy. Smooth out your nights in a way that meets everyone’s needs well enough, get help when you need it, and remember that you and your baby are on the same side in this relationship. Enjoy each other!
For more information on infant and child sleep, see Sweet sleep: nighttime and naptime strategies for the breastfeeding family, by La Leche League International, 2014. Dip into it wherever you like; it covers normal sleep at all ages, details on making your sleeping arrangements safe, naps, the science behind the information, meeting your own sleep needs, your partner’s or support person’s role, sleep-training, talking with your health care provider, and much more.
For breastfeeding help, find a La Leche League Leader here or a certified Lactation Consultant at ilca.org.
LLL Greece Article
FURTHER READING
Sweet Sleep
Infant Sleep
The Safe Sleep Seven
Sleep: Talking With Your Doctor About Bedsharing
Sleep: Safe Surface Checklist
Sleep: Bedshare
Safe Sleep for Breastfeeding Babies
Breast Milk’s Circadian Rhythms
My thoughts about “Sweet Sleep”
REFERENCES
[1] Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome. “SIDS and other sleep-related infant deaths: evidence base for 2016 updated recommendations for a safe infant sleeping environment.” Pediatrics 138, no. 5 (2016): e20162940.
[2]Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome, ibid.
[3] Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome, ibid.
[4] Wiessinger, Diane, Diana West, and Teresa Pitman. Sweet sleep: nighttime and naptime strategies for the breastfeeding family. Ballantine Books, 2014.
[5] Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome, op. cit.
[6] Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome, ibid.
[7] Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome, ibid.
[8] Moon, Rachel Y., and Task Force on Sudden Infant Death Syndrome, ibid.
[9] Hauck, Fern R., John MD Thompson, Kawai O. Tanabe, Rachel Y. Moon, and Mechtild M. Vennemann. “Breastfeeding and reduced risk of sudden infant death syndrome: a meta-analysis.” Pediatrics 128, no. 1 (2011): 103-110.
[10] McKenna, James J., Helen L. Ball, and Lee T. Gettler. “Mother–infant cosleeping, breastfeeding and sudden infant death syndrome: what biological anthropology has discovered about normal infant sleep and pediatric sleep medicine.” American Journal of Physical Anthropology: The Official Publication of the American Association of Physical Anthropologists 134, no. S45 (2007): 133-161.
[11] Wiessinger, Diane, Diana West, and Teresa Pitman. Sweet sleep, op. cit.
[12] McKenna, James J., and Sarah S. Mosko. “Sleep and arousal, synchrony and independence, among mothers and infants sleeping apart and together (same bed): an experiment in evolutionary medicine.” Acta Paediatrica 83 (1994): 94-102.
[13] Machaalani, Rita, and Karen A. Waters. “Neurochemical abnormalities in the brainstem of the sudden infant death syndrome (SIDS).” Paediatric respiratory reviews 15, no. 4 (2014): 293-300.
[14] McKenna, James J., Helen L. Ball, and Lee T. Gettler. “Mother–infant cosleeping, breastfeeding and sudden infant death syndrome: what biological anthropology has discovered about normal infant sleep and pediatric sleep medicine.” American Journal of Physical Anthropology: The Official Publication of the American Association of Physical Anthropologists 134, no. S45 (2007): 133-161.
[15] Gettler, Lee T., and James J. McKenna. “Evolutionary perspectives on mother–infant sleep proximity and breastfeeding in a laboratory setting.” American journal of physical anthropology 144, no. 3 (2011): 454-462.
[16] Waynforth, David. “The influence of parent–infant cosleeping, nursing, and childcare on cortisol and SIgA immunity in a sample of British children.” Developmental Psychobiology: The Journal of the International Society for Developmental Psychobiology 49, no. 6 (2007): 640-648. Tollenaar, M. S., Roseriet Beijers, Jarno Jansen, J. M. A. Riksen-Walraven, and Carolina de Weerth. “Solitary sleeping in young infants is associated with heightened cortisol reactivity to a bathing session but not to a vaccination.” Psychoneuroendocrinology 37, no. 2 (2012): 167-177.
[17] McKenna J, Thomas EB, Anders TF, Sadeh A, Scehchtman VL, Glotzbach SF. Infant -parent co-sleeping in an evolutionary perspective: implications for understanding infant sleep development and the sudden infant death syndrome. Sleep 1993;16:263e82.
[18] Quillin, Stephanie IM, and L. Lee Glenn. “Interaction between feeding method and co‐sleeping on maternal‐newborn sleep.” Journal of Obstetric, Gynecologic, & Neonatal Nursing 33, no. 5 (2004): 580-588.
[19] Ball, Helen L., and Lane E. Volpe. “Sudden Infant Death Syndrome (SIDS) risk reduction and infant sleep location–Moving the discussion forward.” Social science & medicine 79 (2013): 84-91.
[20] Pennestri, Marie-Hélène, Christine Laganière, Andrée-Anne Bouvette-Turcot, Irina Pokhvisneva, Meir Steiner, Michael J. Meaney, and Hélène Gaudreau. “Uninterrupted Infant Sleep, Development, and Maternal Mood.” Pediatrics (2018).
[21] France, Karyn G., Neville M. Blampied, and Jacqueline MT Henderson. “Infant sleep disturbance.” Current Paediatrics 13, no. 3 (2003): 241-246.
[22] Tollenaar, M. S., Roseriet Beijers, Jarno Jansen, J. M. A. Riksen-Walraven, and Carolina de Weerth. “Solitary sleeping in young infants is associated with heightened cortisol reactivity to a bathing session but not to a vaccination.” Psychoneuroendocrinology 37, no. 2 (2012): 167-177.
[23] Middlemiss, Wendy, Douglas A. Granger, Wendy A. Goldberg, and Laura Nathans. “Asynchrony of mother–infant hypothalamic–pituitary–adrenal axis activity following extinction of infant crying responses induced during the transition to sleep.” Early human development 88, no. 4 (2012): 227-232.
[24]Bergman, Nils, in Genna, Catherine Watson. Supporting sucking skills in breastfeeding infants. Jones & Bartlett Learning, 2016.
[25] Ludington-Hoe, Susan, Xiaomei Cong, and Fariba Hashemi. “Infant crying: nature, physiologic consequences, and select interventions.” Neonatal network 21, no. 2 (2002): 29-36.
[26] Maselko, J., L. Kubzansky, L. Lipsitt, and S. L. Buka. “Mother’s affection at 8 months predicts emotional distress in adulthood.” Journal of Epidemiology & Community Health 65, no. 7 (2011): 621-625.
[27] Jenni, Oskar G., and Mary A. Carskadon. “Normal human sleep at different ages: Infants to adolescents.” SRS basics of sleep guide (2005): 11-19.
[28] Coons, Susan, and Christian Guilleminault. “Development of sleep-wake patterns and non-rapid eye movement sleep stages during the first six months of life in normal infants.” Pediatrics 69, no. 6 (1982): 793-798.
[29] Moore, Terence, and L. E. Ucko. “Night waking in early infancy: Part I.” Archives of disease in childhood 32, no. 164 (1957): 333.
[30] McKenna, James J., and Sarah S. Mosko, op. cit.
[31] Moore, Terence, and L. E. Ucko, op. cit.
[32] Goodlin-Jones, Beth L., Melissa M. Burnham, Erika E. Gaylor, and Thomas F. Anders. “Night waking, sleep-wake organization, and self-soothing in the first year of life.” Journal of developmental and behavioral pediatrics: JDBP 22, no. 4 (2001): 226.
[33] Adams, S. M., D. R. Jones, A. Esmail, and E. A. Mitchell. “What affects the age of first sleeping through the night?” Journal of paediatrics and child health 40, no. 3 (2004): 96-101.
[34] Pennestri, et al., op cit. [34] France, Karyn G., Neville M. Blampied, and Jacqueline MT Henderson. “Infant sleep disturbance.” Current Paediatrics 13, no. 3 (2003): 241-246.
[35] Uvnäs Moberg, K., and Danielle K. Prime. “Oxytocin effects in mothers and infants during breastfeeding.” Infant 9, no. 6 (2013): 201-206.
[36] Uvnäs Moberg, Prime, ibid.
[37] Elias, Marjorie F., Nancy A. Nicolson, Carolyn Bora, and Johanna Johnston. “Sleep/wake patterns of breast-fed infants in the first 2 years of life.” Pediatrics 77, no. 3 (1986): 322-329.